Hiss et al in 1960 studied the ECGs of 6014 healthy men in the US Air force. They found that 91% had ST segment elevation of 1mm to 3 mm in one or more precordial leads. This demonstrates the common nature of BER. The incidence of this finding decreases with age. Women demonstrate ST elevation of > 1mm in only 20% of cases and this does not appear to change with increasing age3. It is equally common in all races
BER has elevated upward sloping concave ST segments. This concave (EN HAUT !!!) nature cannot be used as a discriminator on its own but when seen in conjunction with the other features of BER it may be of help. STE due to BER is typically evident in the precordial leads: 74% in V1-V2, 73% in V3-V4 and 37% in inferior lead.
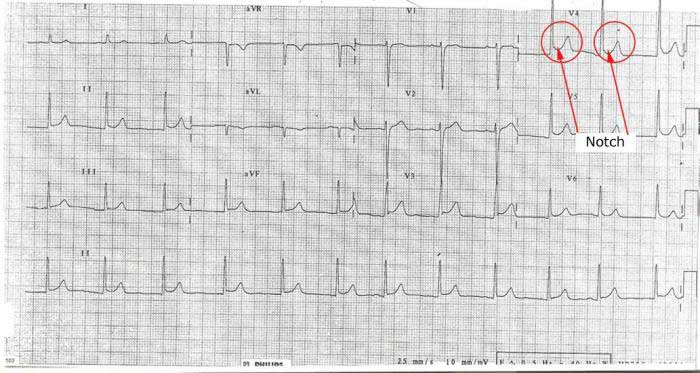
“Notch” or “Slur” at the end of the QRS (at the J point): One of the features seen in BER is an upward sloping notch at the end of the QRS segment.
This is seen more in the precordial leads in BER and is not a feature of pericarditis
A notch at the end of the QRS segment is often seen in BER:
The magnitude of STE can help to differentiate BER from STEMI: one study reported that 57% of ECGs showing ST elevation due to BER was of 1mV amplitude or less; where the amplitude was 5mV or greater it was due to BER in only 2% of cases.